Bridging the gap between study outcomes and real-world results. Algorithm-driven management in a rural cardioMEMS population
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
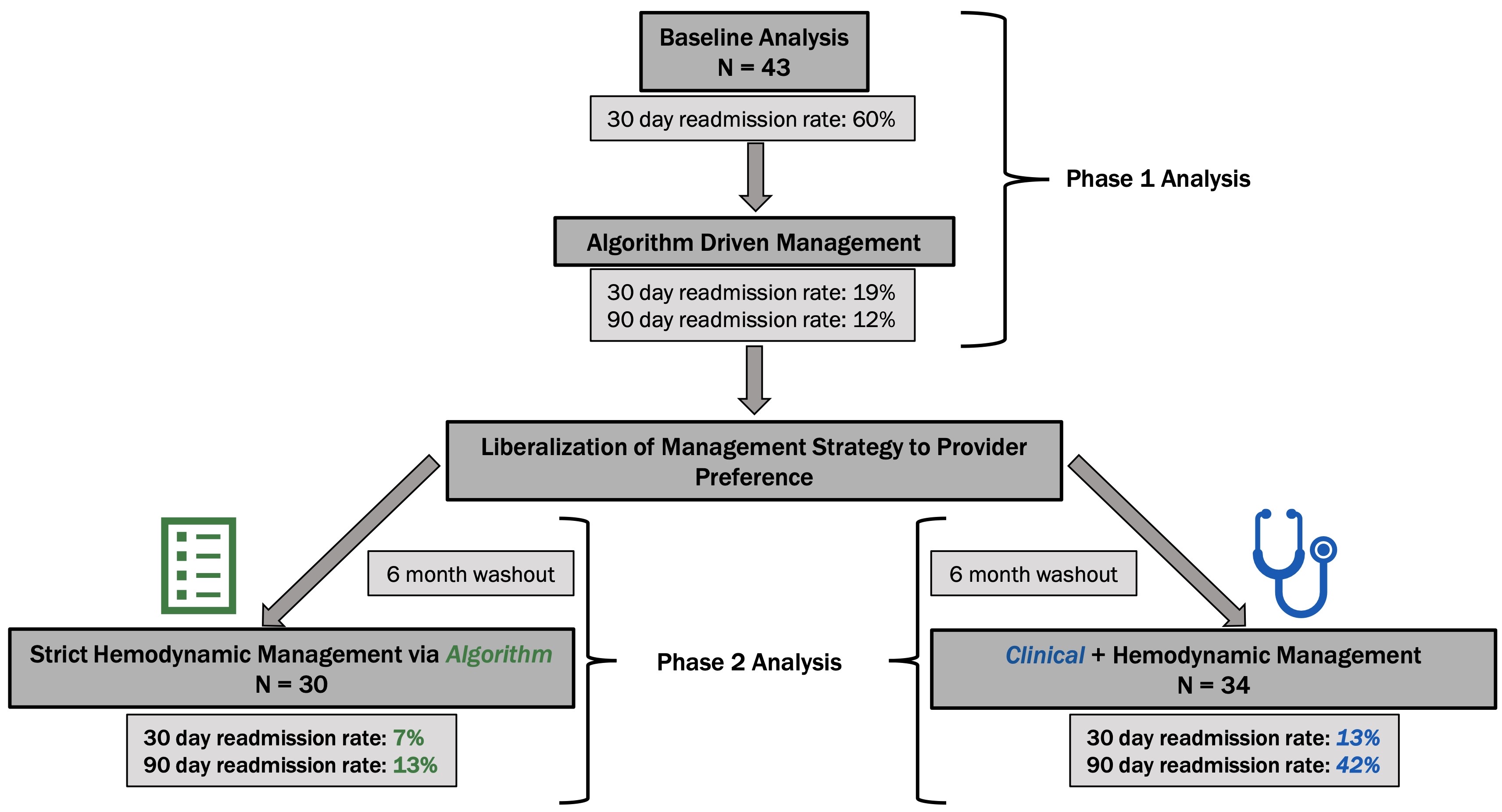
Current therapeutic strategies are ineffective at keeping heart failure patients out of hospital. In 2017, all-cause readmission rates were 19.9% at thirty-days and 34.6% at ninety-days. Large scale studies have shown potential advantages with remote pulmonary artery pressure monitoring. We sought to refine the management of our remotely monitored cohort by introducing a hemodynamic treatment algorithm. A population of rural heart failure patients previously implanted and managed with remote pulmonary artery pressure sensors were studied (n=43). Algorithm based hemodynamic management began with prospective outcome monitoring for ninety days during which algorithm use was mandatory. Following the initial observation period, some physicians reverted to prior practice habit which included consideration of standard heart failure metrics into decision making. Following a six-month washout period, retrospective analysis was performed in evaluation of the intervention arm (n=34), patients managed by hemodynamic plus usual heart failure data, and the control group (n=30), those who remained strictly managed by algorithm. Pre-algorithm thirty-day heart failure specific hospitalization (HFH) rate was 60%. Algorithm-driven management decreased HFH rates to 19% at thirty-days and 12% at ninety-days. Incorporating standard heart failure metrics with remotely pulmonary artery (PA) pressure data markedly increased risk of readmission (7% vs 13% at thirty-days and 13% vs 42% at ninety-days). Heart failure patients managed via remote pulmonary artery pressures benefitted from algorithm-driven hemodynamic therapies. Utility and effectiveness of remote PA monitoring is stunted with consideration of traditional heart failure metrics (weights, symptoms, exam findings) in their management.
Graphical Abstract




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- Adeseye A. Akintunde, Sope T. Orugun, The association of iron deficiency with right ventricular dysfunction in Africans with heart failure , Global Cardiology: Vol. 2 No. 4 (2024)
- Sven Christopher Aland, Christoph Gertler, Hannah Leonie Bräunig, Timo Schröder, Frank Edelmann, Rolf Wachter, Christoph Herrmann-Lingen, Gerd Hasenfuß, Anja Sandek, Exercise capacity, iron deficiency and depressive symptoms in patients with asymptomatic chronic systolic heart failure , Global Cardiology: Vol. 2 No. 2 (2024)
- Khawaja M. Talha, Javed Butler, Stephan von Haehling, Mitja Lainscak, Piotr Ponikowski, Stefan D. Anker, Defining iron replete status in patients with heart failure treated with intravenous iron , Global Cardiology: Vol. 1 No. 1 (2023)
- Jelena Čelutkienė, Agnė Monika Jakštaitė, Jolita Badarienė, Svetlana Solovjova, Ieva Slivovskaja, Rokas Navickas, Edita Kazėnaitė, Egidija Rinkūnienė, Alma Čypienė, Jonas Misiūra, Ligita Ryliškytė, Aleksandras Laucevičius, Andrew J.S. Coats, Detection of early heart failure with preserved ejection fraction in metabolic syndrome patients detected as part of a national screening program in middle aged subjects , Global Cardiology: Vol. 1 No. 1 (2023)
- Muhammad Shariq Usman, Arsalan Hamid, Shurjeel Uddin Qazi, Mikhail N. Kosiborod, Deepak L. Bhatt, Muhammad Shahzeb Khan, Muthiah Vaduganathan, Javed Butler, The effect of SGLT2 inhibitors on health status in patients with heart failure: a systematic review and meta-analysis , Global Cardiology: Vol. 2 No. 2 (2024)
- Muhammad Shahzeb Khan, Javed Butler, Laibah Arshad Khan, Markus S. Anker, Advanced cancer as a heart failure like syndrome due to cardiac wasting cardiomyopathy: facts and numbers , Global Cardiology: Vol. 2 No. 4 (2024)
- Maryanne Caruana, Miriam Gatt, Oscar Aquilina, Charles Savona Ventura, Victor Grech, Jane Somerville, The impact of maternal congenital heart disease on pregnancy outcomes in Malta: a retrospective study , Global Cardiology: Vol. 1 No. 1 (2023)
- Stefan D. Anker, Javed Butler, Khawaja M. Talha, Tim Friede, Using multiple primary endpoints in clinical trials with a focus on heart failure , Global Cardiology: Vol. 2 No. 2 (2024)
- Kamilu M. Karaye, Abdulrazaq G. Habib, Karen Sliwa, Epidemiology of peripartum cardiomyopathy in Africa , Global Cardiology: Vol. 2 No. 2 (2024)
- Maryanne Caruana, Philip Moons, Adrienne H. Kovacs, Koen Luyckx, Corina Thomet, Werner Budts, Maayke Sluman, Katrine Eriksen, Mikael Dellborg, Malin Berghammer, Bengt Johansson, Alexandra Soufi, Edward Callus, Victor Grech, Silke Apers, Quality of life in Maltese adults with congenital heart disease: a second look , Global Cardiology: Vol. 2 No. 1 (2024)
You may also start an advanced similarity search for this article.